
Medically reviewed by Dr. Maryam Jahanshahi, ND· Last updated July 2026 · 9 min read
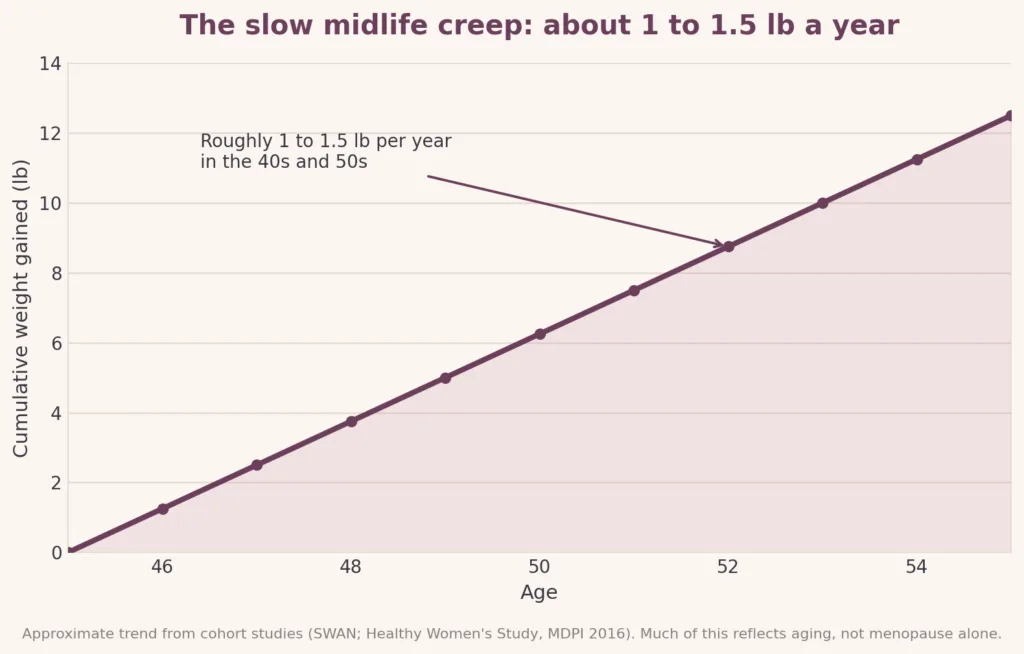
The short answer: Perimenopause weight gain is real, and it is not a willpower problem. Most women gain about one to one and a half pounds a year through their 40s and 50s. Much of that gradual gain is driven by aging and lifestyle, but the shift of fat toward the belly and the faster loss of muscle are driven by falling estrogen. Protecting muscle is the single most effective response.
If you have hit your mid-40s and noticed that the eating and exercise habits that used to keep your weight steady suddenly are not working, and that the weight seems to be settling around your middle in a way it never did before, you are not imagining it.
Perimenopause weight gain is one of the most common and least talked-about parts of the menopause transition. It is also one of the most misunderstood. During these years, your body genuinely changes how it stores fat, builds muscle, and burns energy. The old playbook stops working because the biology underneath it has changed.
The good news: once you understand what is changing, the picture becomes much less mysterious and much more workable. Let us walk through it the way we would if you were sitting across from us at our clinic in Ajax.
Key takeaways
- Weight gain during perimenopause is common, biological, and not a discipline problem.
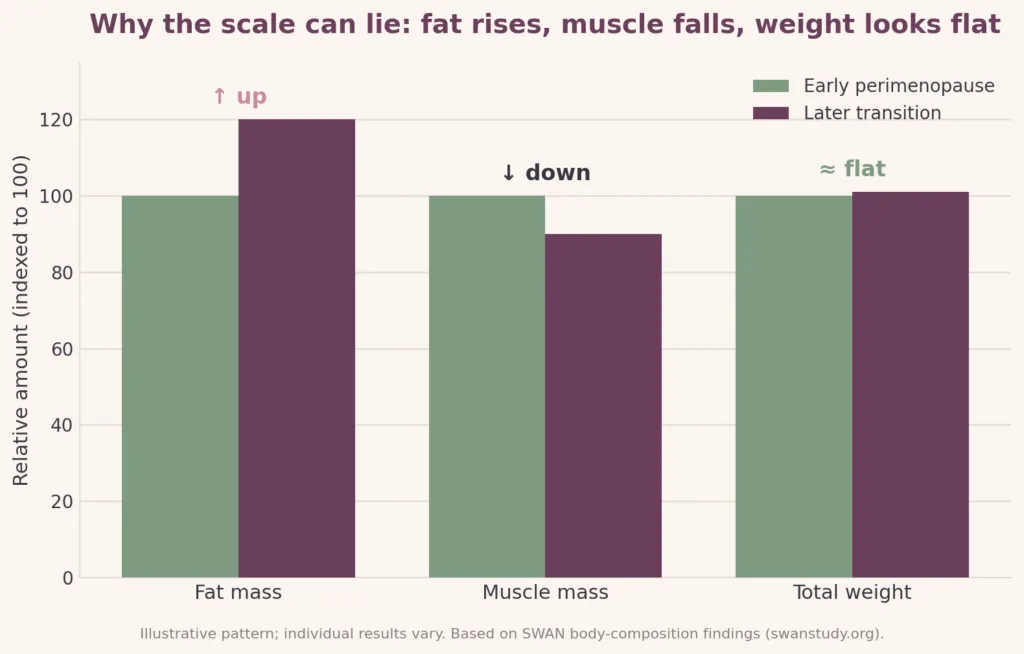
- The scale can under-report what is happening because you may be losing muscle while gaining fat.
- Falling estrogen shifts fat toward the abdomen, including deep visceral fat.
- Protecting muscle with protein and strength training is the highest-value strategy.
- Hormone therapy does not cause weight gain, but it is not a weight-loss treatment either.
- An individualized medical assessment beats generic advice.

What is perimenopause?
Perimenopause is the transition leading up to menopause, the years when your ovaries gradually shift how they produce hormones. It usually begins in your early-to-mid 40s, though it can start earlier, and it can last anywhere from a few years to a decade.
The key word is transition. Hormones like estrogen do not simply switch off. They fluctuate, sometimes wildly, before they eventually settle at lower levels. That up-and-down pattern is why symptoms feel so unpredictable from one month to the next, and it is a big part of why your metabolism can feel like it is working against you..
How much weight do women actually gain during perimenopause?
Most women gain roughly one to one and a half pounds per year through their 40s and 50s. Across the whole transition, that adds up to somewhere around ten to fifteen pounds for many women, though the range is wide and some women gain little or none at all.
Two things are worth knowing about that number.
First, the number on the scale is mostly an aging story. Large studies of women moving through midlife, including the long-running Study of Women’s Health Across the Nation (SWAN), found that this gradual creep is tied largely to normal aging and lifestyle rather than to menopause specifically. SWAN found no clear acceleration in the rate of weight gain during the transition itself.
Second, the scale is not the whole story. Which brings us to the part most articles skip.
Why does perimenopause cause belly fat?
Even when the scale barely moves, what your body is made of shifts. As estrogen declines, fat tends to redistribute away from the hips and thighs and toward the abdomen. That includes visceral fat, the deeper fat stored around your internal organs, which matters more for your health than the fat you can pinch.
One review of the research found that visceral fat can climb from about 5 to 8 percent of total body fat before menopause to roughly 15 to 20 percent afterward.

This is what people mean by “menopause belly.” It is a real change in body composition, even if your clothes size does not tell the whole story. So if your body feels like it is behaving differently even though the scale is only creeping, you are reading it correctly. The distribution is changing, not just the total.
Why the scale can lie: the muscle-for-fat swap
Here is the detail that explains most of the confusion.
During the menopause transition, two things happen at once: you tend to gain fat and lose muscle. Because muscle is denser than fat, these changes can partly cancel each other out on the scale. That is why some women gain very little weight but still watch their bodies reshape, and their clothes fit differently.
The muscle loss matters more than most people realize. We all steadily lose some muscle from our 30s onward, but the menopausal transition appears to accelerate it. Research suggests falling estrogen tips the balance toward muscle breakdown and makes muscle less responsive to the protein we eat, a kind of “anabolic resistance,” meaning the body does not build muscle from food as efficiently as it once did.
Why care about muscle if your goal is weight? Because muscle is metabolically active tissue. It is a major part of what determines how many calories you burn at rest, your resting metabolic rate. Lose muscle, and your resting metabolism quietly drops. Suddenly, the amount of food that used to maintain your weight is a little too much, through no change in your habits at all.
During perimenopause, protecting your muscles is protecting your metabolism.
What else makes weight loss harder: insulin, sleep, and cortisol
Perimenopause weight gain is not only about estrogen. Three other players make it harder:
Insulin sensitivity. Estrogen helps your body respond to insulin, the hormone that manages blood sugar. As estrogen becomes less stable, many women find their bodies handle carbohydrates less efficiently, which can make fat storage around the middle easier.
Sleep. Sleep disruption is extremely common in perimenopause. Hot flashes and night sweats fragment sleep, and poor sleep is strongly linked to increased appetite, stronger cravings, and higher stress hormones the next day.
Cortisol and stress. Midlife piles on demanding careers, growing kids, and aging parents at exactly the time hormonal shifts can make the nervous system more reactive to stress. Higher, sustained cortisol tends to encourage fat storage around the abdomen.
None of these are moral failings. They are physiological, and most of them are things a good plan can actually address.
Three myths about perimenopause weight gain
Myth: “Hormone therapy will make me gain weight.” The evidence does not support it. A Cochrane review, one of the most rigorous types of evidence review there is, found no evidence that hormone therapy causes weight gain beyond what women typically gain at menopause anyway. It also found that hormone therapy does not prevent that weight gain, so it is not a weight-loss treatment. Whether hormone therapy is right for you is an individual decision to make with a clinician, but “it will make me gain weight” should not be the deciding factor.
Myth: “I just need to eat less and move more, as I used to.” Eating well and moving matter enormously, but doing exactly what worked at 35 often is not enough at 50, because the underlying muscle and metabolism picture has changed. The strategy needs to shift toward protecting muscle, not just cutting calories.
Myth: “This is permanent, and there is nothing I can do.” Not true. The biology is real, but it is not a locked door.
What actually helps with perimenopause weight gain
There’s no single fix, but the evidence points consistently in a few directions:
Prioritize protein and resistance training. Because the core problem is muscle loss and anabolic resistance, strength training and adequate dietary protein are arguably more important now than at any earlier stage of life. This is the lever with the biggest payoff.
Protect your sleep. Addressing sleep disruption, including the menopausal symptoms causing it, quietly improves appetite regulation and stress hormones.
Manage stress realistically. Not a spa-day platitude: practical, sustainable stress management genuinely influences where your body stores fat.
Work with a dietitian rather than a diet. Generic calorie targets tend to under-deliver protein at exactly the stage of life when protein matters most.
Get an individualized medical assessment. For some women, the right plan may include menopausal hormone therapy for symptoms, or, where clinically appropriate and after a proper assessment, medically supervised weight management. These are individual decisions that depend on your health history, and they belong in a conversation with a qualified clinician. (Related: what to expect at your first metabolic health consultation)
Who might benefit from medical support?
You don’t need to white-knuckle this alone. It may be worth speaking to a healthcare professional if you’re noticing:
- Weight or body-composition changes that aren’t responding to your usual approach
- New concentration of weight around your midsection
- Perimenopausal symptoms (hot flashes, sleep problems, mood changes) that are affecting your quality of life
- A personal or family history of diabetes, heart disease, or metabolic conditions
- A sense that you want a plan built around your body rather than generic advice
When to seek medical advice sooner
Some signs deserve prompt attention rather than watchful waiting: rapid or unexplained weight change, symptoms significantly disrupting your daily life, or any new or worsening health concerns. A clinician can help rule out other causes, such as thyroid conditions, and make sure you get the right assessment.
Frequently asked questions
The bottom line
If your body feels like it’s playing by new rules, that’s because it is. Perimenopause changes your metabolism, your muscles, and where you store fat. Understanding those changes is the first step toward working with your body rather than against it. You haven’t failed. The approach just needs to catch up with the biology.
Talk to our team. Aniyah Care offers metabolic health assessments for women in Ajax and across Durham Region who are navigating this exact stage of life. If you would like a plan built around your body and your health history, book a metabolic health consultation.
References
1. SWAN, Study of Women’s Health Across the Nation. *Changes in Body Composition and Weight During the Menopause Transition.* https://www.swanstudy.org/changes-in-body-composition-and-weight-during-the-menopause-transition/
2. Ambikairajah A, et al. *Adverse Changes in Body Composition During the Menopausal Transition and Relation to Cardiovascular Risk: A Contemporary Review.* https://pmc.ncbi.nlm.nih.gov/articles/PMC9258798/
3. Simpson SJ, et al. *Weight gain during the menopause transition: Evidence for a mechanism dependent on protein leverage.* BJOG, 2023. https://doi.org/10.1111/1471-0528.17290
4. Kongnyuy EJ, et al. *Hormone replacement therapy has no effect on body weight and cannot prevent weight gain at menopause* (Cochrane review, CD001018). https://www.cochrane.org/evidence/CD001018_hormone-replacement-therapy-has-no-effect-body-weight-and-cannot-prevent-weight-gain-menopause
5. Davis SR, et al. *Association of Mid-Life Changes in Body Size, Body Composition and Obesity Status with the Menopausal Transition.* Healthcare (MDPI), 2016. https://www.mdpi.com/2227-9032/4/3/42
6. Troia L, et al. *Sleep Disturbance and Perimenopause: A Narrative Review.* J Clin Med, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11901009/







